
11 Mar 2025
nnInteractive introduces a comprehensive framework for interactive 3D medical image segmentation, designed to overcome limitations of 2D-focused approaches and enhance real-world applicability. It achieves true volumetric consistency, supports diverse 3D interaction types across multiple axes, generalizes across 120+ modalities, and enables radiologists to complete segmentations 72% faster while maintaining expert-level quality.

18 Apr 2025
The field of self-supervised learning (SSL) for 3D medical images lacks
consistency and standardization. While many methods have been developed, it is
impossible to identify the current state-of-the-art, due to i) varying and
small pretraining datasets, ii) varying architectures, and iii) being evaluated
on differing downstream datasets. In this paper, we bring clarity to this field
and lay the foundation for further method advancements through three key
contributions: We a) publish the largest publicly available pre-training
dataset comprising 114k 3D brain MRI volumes, enabling all practitioners to
pre-train on a large-scale dataset. We b) benchmark existing 3D self-supervised
learning methods on this dataset for a state-of-the-art CNN and Transformer
architecture, clarifying the state of 3D SSL pre-training. Among many findings,
we show that pre-trained methods can exceed a strong from-scratch nnU-Net
ResEnc-L baseline. Lastly, we c) publish the code of our pre-training and
fine-tuning frameworks and provide the pre-trained models created during the
benchmarking process to facilitate rapid adoption and reproduction.
28 Feb 2025

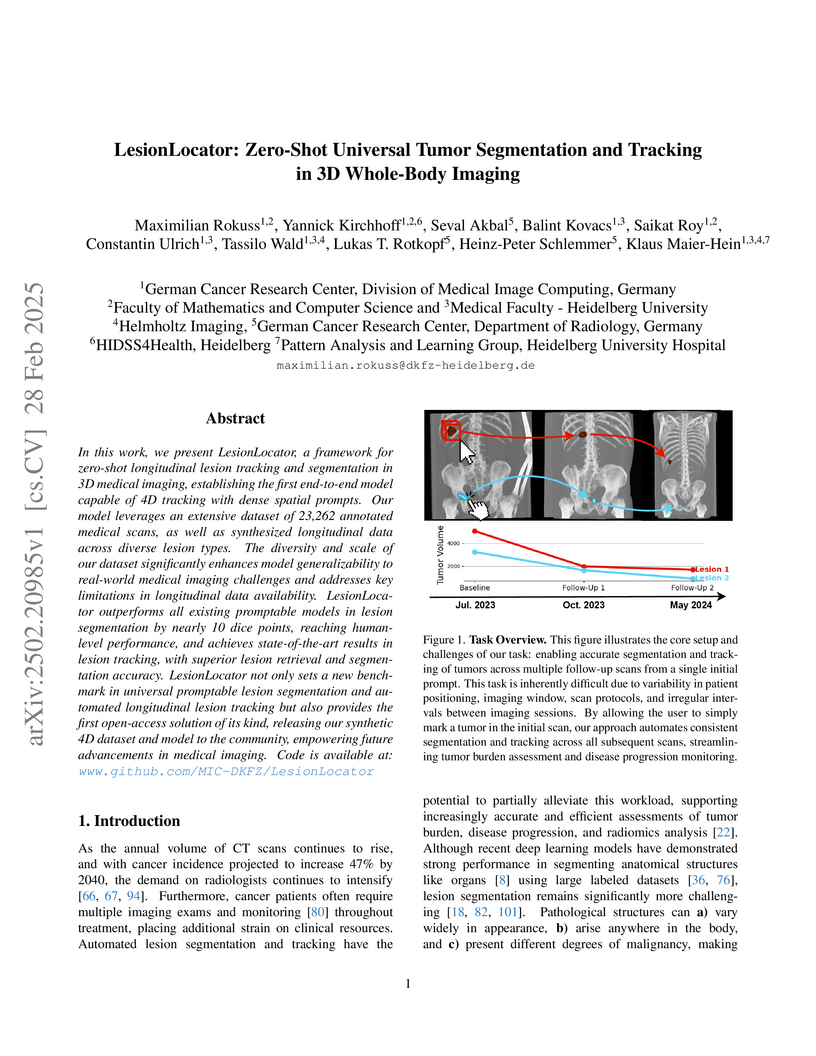
In this work, we present LesionLocator, a framework for zero-shot
longitudinal lesion tracking and segmentation in 3D medical imaging,
establishing the first end-to-end model capable of 4D tracking with dense
spatial prompts. Our model leverages an extensive dataset of 23,262 annotated
medical scans, as well as synthesized longitudinal data across diverse lesion
types. The diversity and scale of our dataset significantly enhances model
generalizability to real-world medical imaging challenges and addresses key
limitations in longitudinal data availability. LesionLocator outperforms all
existing promptable models in lesion segmentation by nearly 10 dice points,
reaching human-level performance, and achieves state-of-the-art results in
lesion tracking, with superior lesion retrieval and segmentation accuracy.
LesionLocator not only sets a new benchmark in universal promptable lesion
segmentation and automated longitudinal lesion tracking but also provides the
first open-access solution of its kind, releasing our synthetic 4D dataset and
model to the community, empowering future advancements in medical imaging. Code
is available at: www.github.com/MIC-DKFZ/LesionLocator

10 Apr 2025
Landmark detection plays a crucial role in medical imaging tasks that rely on
precise spatial localization, including specific applications in diagnosis,
treatment planning, image registration, and surgical navigation. However,
manual annotation is labor-intensive and requires expert knowledge. While deep
learning shows promise in automating this task, progress is hindered by limited
public datasets, inconsistent benchmarks, and non-standardized baselines,
restricting reproducibility, fair comparisons, and model generalizability. This
work introduces nnLandmark, a self-configuring deep learning framework for 3D
medical landmark detection, adapting nnU-Net to perform heatmap-based
regression. By leveraging nnU-Net's automated configuration, nnLandmark
eliminates the need for manual parameter tuning, offering out-of-the-box
usability. It achieves state-of-the-art accuracy across two public datasets,
with a mean radial error (MRE) of 1.5 mm on the Mandibular Molar Landmark (MML)
dental CT dataset and 1.2 mm for anatomical fiducials on a brain MRI dataset
(AFIDs), where nnLandmark aligns with the inter-rater variability of 1.5 mm.
With its strong generalization, reproducibility, and ease of deployment,
nnLandmark establishes a reliable baseline for 3D landmark detection,
supporting research in anatomical localization and clinical workflows that
depend on precise landmark identification. The code will be available soon.

05 Aug 2025
Digital pathology has seen the advent of a wealth of foundational models (FM), yet to date their performance on cell phenotyping has not been benchmarked in a unified manner. We therefore propose PhenoBench: A comprehensive benchmark for cell phenotyping on Hematoxylin and Eosin (H&E) stained histopathology images. We provide both PhenoCell, a new H&E dataset featuring 14 granular cell types identified by using multiplexed imaging, and ready-to-use fine-tuning and benchmarking code that allows the systematic evaluation of multiple prominent pathology FMs in terms of dense cell phenotype predictions in different generalization scenarios. We perform extensive benchmarking of existing FMs, providing insights into their generalization behavior under technical vs. medical domain shifts. Furthermore, while FMs achieve macro F1 scores > 0.70 on previously established benchmarks such as Lizard and PanNuke, on PhenoCell, we observe scores as low as 0.20. This indicates a much more challenging task not captured by previous benchmarks, establishing PhenoCell as a prime asset for future benchmarking of FMs and supervised models alike. Code and data are available on GitHub.

19 Sep 2025
Large-scale pre-training holds the promise to advance 3D medical object detection, a crucial component of accurate computer-aided diagnosis. Yet, it remains underexplored compared to segmentation, where pre-training has already demonstrated significant benefits. Existing pre-training approaches for 3D object detection rely on 2D medical data or natural image pre-training, failing to fully leverage 3D volumetric information. In this work, we present the first systematic study of how existing pre-training methods can be integrated into state-of-the-art detection architectures, covering both CNNs and Transformers. Our results show that pre-training consistently improves detection performance across various tasks and datasets. Notably, reconstruction-based self-supervised pre-training outperforms supervised pre-training, while contrastive pre-training provides no clear benefit for 3D medical object detection. Our code is publicly available at: this https URL.

21 Feb 2025
Reliable evaluation of AI models is critical for scientific progress and
practical application. While existing VLM benchmarks provide general insights
into model capabilities, their heterogeneous designs and limited focus on a few
imaging domains pose significant challenges for both cross-domain performance
comparison and targeted domain-specific evaluation. To address this, we propose
three key contributions: (1) a framework for the resource-efficient creation of
domain-specific VLM benchmarks enabled by task augmentation for creating
multiple diverse tasks from a single existing task, (2) the release of new VLM
benchmarks for seven domains, created according to the same homogeneous
protocol and including 162,946 thoroughly human-validated answers, and (3) an
extensive benchmarking of 22 state-of-the-art VLMs on a total of 37,171 tasks,
revealing performance variances across domains and tasks, thereby supporting
the need for tailored VLM benchmarks. Adoption of our methodology will pave the
way for the resource-efficient domain-specific selection of models and guide
future research efforts toward addressing core open questions.
20 Jan 2025
Touchstone Benchmark: Are We on the Right Way for Evaluating AI Algorithms for Medical Segmentation?
Touchstone Benchmark: Are We on the Right Way for Evaluating AI Algorithms for Medical Segmentation?


How can we test AI performance? This question seems trivial, but it isn't. Standard benchmarks often have problems such as in-distribution and small-size test sets, oversimplified metrics, unfair comparisons, and short-term outcome pressure. As a consequence, good performance on standard benchmarks does not guarantee success in real-world scenarios. To address these problems, we present Touchstone, a large-scale collaborative segmentation benchmark of 9 types of abdominal organs. This benchmark is based on 5,195 training CT scans from 76 hospitals around the world and 5,903 testing CT scans from 11 additional hospitals. This diverse test set enhances the statistical significance of benchmark results and rigorously evaluates AI algorithms across various out-of-distribution scenarios. We invited 14 inventors of 19 AI algorithms to train their algorithms, while our team, as a third party, independently evaluated these algorithms on three test sets. In addition, we also evaluated pre-existing AI frameworks--which, differing from algorithms, are more flexible and can support different algorithms--including MONAI from NVIDIA, nnU-Net from DKFZ, and numerous other open-source frameworks. We are committed to expanding this benchmark to encourage more innovation of AI algorithms for the medical domain.
29 Aug 2025
Automated segmentation of Pancreatic Ductal Adenocarcinoma (PDAC) from MRI is critical for clinical workflows but is hindered by poor tumor-tissue contrast and a scarcity of annotated data. This paper details our submission to the PANTHER challenge, addressing both diagnostic T1-weighted (Task 1) and therapeutic T2-weighted (Task 2) segmentation. Our approach is built upon the nnU-Net framework and leverages a deep, multi-stage cascaded pre-training strategy, starting from a general anatomical foundation model and sequentially fine-tuning on CT pancreatic lesion datasets and the target MRI modalities. Through extensive five-fold cross-validation, we systematically evaluated data augmentation schemes and training schedules. Our analysis revealed a critical trade-off, where aggressive data augmentation produced the highest volumetric accuracy, while default augmentations yielded superior boundary precision (achieving a state-of-the-art MASD of 5.46 mm and HD95 of 17.33 mm for Task 1). For our final submission, we exploited this finding by constructing custom, heterogeneous ensembles of specialist models, essentially creating a mix of experts. This metric-aware ensembling strategy proved highly effective, achieving a top cross-validation Tumor Dice score of 0.661 for Task 1 and 0.523 for Task 2. Our work presents a robust methodology for developing specialized, high-performance models in the context of limited data and complex medical imaging tasks (Team MIC-DKFZ).
25 Aug 2025
These lecture notes evolve around mathematical concepts arising in inverse problems. We start by introducing inverse problems through examples such as differentiation, deconvolution, computed tomography and phase retrieval. This then leads us to the framework of well-posedness and first considerations regarding reconstruction and inversion approaches. The second chapter then first deals with classical regularization theory of inverse problems in Hilbert spaces. After introducing the pseudo-inverse, we review the concept of convergent regularization. Within this chapter we then proceed to ask the question of how to realize practical reconstruction algorithms. Here, we mainly focus on Tikhonov and sparsity promoting regularization in finite dimensional spaces. In the third chapter, we dive into modern deep-learning methods, which allow solving inverse problems in a data-dependent approach. The intersection between inverse problems and machine learning is a rapidly growing field and our exposition here restricts itself to a very limited selection of topics. Among them are learned regularization, fully-learned Bayesian estimation, post-processing strategies and plug-n-play methods.
05 Nov 2025
 CNRS
CNRS University of CambridgeHeidelberg University
University of CambridgeHeidelberg University Imperial College LondonUniversity of Zurich
Imperial College LondonUniversity of Zurich University College London
University College London The Chinese University of Hong Kong
The Chinese University of Hong Kong University of PennsylvaniaTUD Dresden University of Technology
University of PennsylvaniaTUD Dresden University of Technology Sorbonne Université
Sorbonne Université InriaHelmholtz-Zentrum Dresden-Rossendorf (HZDR)INSERMHelmholtz-Zentrum Dresden-RossendorfUniversity Hospital CologneWestern UniversityGerman Cancer Research CenterHeidelberg University HospitalUniversity of StrasbourgNational Center for Tumor Diseases (NCT)Lawson Health Research InstituteHelmholtz ImagingAP-HPInstitut du Cerveau – Paris Brain Institute - ICMBalgrist University HospitalChildren’s National HospitalReutlingen UniversityGerman Cancer Research Center (DKFZ) HeidelbergUCL Hawkes InstituteUniversity College London HospitalNational Center for Tumor DiseasesEnAcuity Ltd.University Hospital LeipzigHIDSS4Health - Helmholtz Information and Data Science School for HealthHôpital de la Pitié SalpêtrièreHI Helmholtz ImagingElse Kröner Fresenius Center for Digital HealthFaculty of Medicine and University Hospital Carl Gustav CarusAI Health Innovation ClusterUniversity Medical Center HeidelbergAP-HP, Hôpital de la Pitié-SalpêtrièreScialyticsDZHK Partnersite Heidelberg-MannheimVerb Surgical Inc.Children
DANQueens
’ University
InriaHelmholtz-Zentrum Dresden-Rossendorf (HZDR)INSERMHelmholtz-Zentrum Dresden-RossendorfUniversity Hospital CologneWestern UniversityGerman Cancer Research CenterHeidelberg University HospitalUniversity of StrasbourgNational Center for Tumor Diseases (NCT)Lawson Health Research InstituteHelmholtz ImagingAP-HPInstitut du Cerveau – Paris Brain Institute - ICMBalgrist University HospitalChildren’s National HospitalReutlingen UniversityGerman Cancer Research Center (DKFZ) HeidelbergUCL Hawkes InstituteUniversity College London HospitalNational Center for Tumor DiseasesEnAcuity Ltd.University Hospital LeipzigHIDSS4Health - Helmholtz Information and Data Science School for HealthHôpital de la Pitié SalpêtrièreHI Helmholtz ImagingElse Kröner Fresenius Center for Digital HealthFaculty of Medicine and University Hospital Carl Gustav CarusAI Health Innovation ClusterUniversity Medical Center HeidelbergAP-HP, Hôpital de la Pitié-SalpêtrièreScialyticsDZHK Partnersite Heidelberg-MannheimVerb Surgical Inc.Children
DANQueens
’ UniversitySurgical data science (SDS) is rapidly advancing, yet clinical adoption of artificial intelligence (AI) in surgery remains severely limited, with inadequate validation emerging as a key obstacle. In fact, existing validation practices often neglect the temporal and hierarchical structure of intraoperative videos, producing misleading, unstable, or clinically irrelevant results. In a pioneering, consensus-driven effort, we introduce the first comprehensive catalog of validation pitfalls in AI-based surgical video analysis that was derived from a multi-stage Delphi process with 91 international experts. The collected pitfalls span three categories: (1) data (e.g., incomplete annotation, spurious correlations), (2) metric selection and configuration (e.g., neglect of temporal stability, mismatch with clinical needs), and (3) aggregation and reporting (e.g., clinically uninformative aggregation, failure to account for frame dependencies in hierarchical data structures). A systematic review of surgical AI papers reveals that these pitfalls are widespread in current practice, with the majority of studies failing to account for temporal dynamics or hierarchical data structure, or relying on clinically uninformative metrics. Experiments on real surgical video datasets provide the first empirical evidence that ignoring temporal and hierarchical data structures can lead to drastic understatement of uncertainty, obscure critical failure modes, and even alter algorithm rankings. This work establishes a framework for the rigorous validation of surgical video analysis algorithms, providing a foundation for safe clinical translation, benchmarking, regulatory review, and future reporting standards in the field.
30 Aug 2025
Accurate segmentation of lesions in longitudinal whole-body CT is essential for monitoring disease progression and treatment response. While automated methods benefit from incorporating longitudinal information, they remain limited in their ability to consistently track individual lesions across time. Task 2 of the autoPET/CT IV Challenge addresses this by providing lesion localizations and baseline delineations, framing the problem as longitudinal promptable segmentation. In this work, we extend the recently proposed LongiSeg framework with promptable capabilities, enabling lesion-specific tracking through point and mask interactions. To address the limited size of the provided training set, we leverage large-scale pretraining on a synthetic longitudinal CT dataset. Our experiments show that pretraining substantially improves the ability to exploit longitudinal context, yielding an improvement of up to 6 Dice points compared to models trained from scratch. These findings demonstrate the effectiveness of combining longitudinal context with interactive prompting for robust lesion tracking. Code is publicly available at this https URL.

03 Apr 2025
 UCLA
UCLA Chinese Academy of Sciences
Chinese Academy of Sciences University of Science and Technology of China
University of Science and Technology of China Beihang UniversityUniversity of WarsawXiamen University
Beihang UniversityUniversity of WarsawXiamen University Johns Hopkins UniversityShenzhen UniversityGerman Cancer Research Center (DKFZ)Warsaw University of TechnologyAGH University of KrakowHelmholtz ImagingFriedrich-Alexander University Erlangen-NurembergBeijing Jishuitan HospitalMedApp S.A.Beijing Rossum Robot Technology Co., Ltd.
Johns Hopkins UniversityShenzhen UniversityGerman Cancer Research Center (DKFZ)Warsaw University of TechnologyAGH University of KrakowHelmholtz ImagingFriedrich-Alexander University Erlangen-NurembergBeijing Jishuitan HospitalMedApp S.A.Beijing Rossum Robot Technology Co., Ltd.The segmentation of pelvic fracture fragments in CT and X-ray images is
crucial for trauma diagnosis, surgical planning, and intraoperative guidance.
However, accurately and efficiently delineating the bone fragments remains a
significant challenge due to complex anatomy and imaging limitations. The
PENGWIN challenge, organized as a MICCAI 2024 satellite event, aimed to advance
automated fracture segmentation by benchmarking state-of-the-art algorithms on
these complex tasks. A diverse dataset of 150 CT scans was collected from
multiple clinical centers, and a large set of simulated X-ray images was
generated using the DeepDRR method. Final submissions from 16 teams worldwide
were evaluated under a rigorous multi-metric testing scheme. The top-performing
CT algorithm achieved an average fragment-wise intersection over union (IoU) of
0.930, demonstrating satisfactory accuracy. However, in the X-ray task, the
best algorithm attained an IoU of 0.774, highlighting the greater challenges
posed by overlapping anatomical structures. Beyond the quantitative evaluation,
the challenge revealed methodological diversity in algorithm design. Variations
in instance representation, such as primary-secondary classification versus
boundary-core separation, led to differing segmentation strategies. Despite
promising results, the challenge also exposed inherent uncertainties in
fragment definition, particularly in cases of incomplete fractures. These
findings suggest that interactive segmentation approaches, integrating human
decision-making with task-relevant information, may be essential for improving
model reliability and clinical applicability.
02 Jun 2025
Heidelberg University Stanford UniversityIT University of Copenhagen
Stanford UniversityIT University of Copenhagen University of CopenhagenCONICET
University of CopenhagenCONICET Emory UniversityAarhus UniversityThe Hebrew University of JerusalemUniversitat de BarcelonaTechnical University of Denmark
Emory UniversityAarhus UniversityThe Hebrew University of JerusalemUniversitat de BarcelonaTechnical University of Denmark University of GroningenUniversity of Southern DenmarkRadboud University Medical CenterGerman Cancer Research CenterRigshospitaletARTORG Center for Biomedical Engineering Research, University of BernUniversity of Buenos AiresHelmholtz ImagingLunitFederal University of Espírito SantoCopenhagen University Hospital, Herlev and GentofteCerebriu A/SChurchill Hospital, Oxford University HospitalsSteno Diabetes Center Aarhus, Aarhus University HospitalUniversity Hospital Bern, University of BernEurécom
University of GroningenUniversity of Southern DenmarkRadboud University Medical CenterGerman Cancer Research CenterRigshospitaletARTORG Center for Biomedical Engineering Research, University of BernUniversity of Buenos AiresHelmholtz ImagingLunitFederal University of Espírito SantoCopenhagen University Hospital, Herlev and GentofteCerebriu A/SChurchill Hospital, Oxford University HospitalsSteno Diabetes Center Aarhus, Aarhus University HospitalUniversity Hospital Bern, University of BernEurécom
Stanford UniversityIT University of CopenhagenUniversity of CopenhagenCONICETEmory UniversityAarhus UniversityThe Hebrew University of JerusalemUniversitat de BarcelonaTechnical University of DenmarkUniversity of GroningenUniversity of Southern DenmarkRadboud University Medical CenterGerman Cancer Research CenterRigshospitaletARTORG Center for Biomedical Engineering Research, University of BernUniversity of Buenos AiresHelmholtz ImagingLunitFederal University of Espírito SantoCopenhagen University Hospital, Herlev and GentofteCerebriu A/SChurchill Hospital, Oxford University HospitalsSteno Diabetes Center Aarhus, Aarhus University HospitalUniversity Hospital Bern, University of BernEurécomDatasets play a critical role in medical imaging research, yet issues such as label quality, shortcuts, and metadata are often overlooked. This lack of attention may harm the generalizability of algorithms and, consequently, negatively impact patient outcomes. While existing medical imaging literature reviews mostly focus on machine learning (ML) methods, with only a few focusing on datasets for specific applications, these reviews remain static -- they are published once and not updated thereafter. This fails to account for emerging evidence, such as biases, shortcuts, and additional annotations that other researchers may contribute after the dataset is published. We refer to these newly discovered findings of datasets as research artifacts. To address this gap, we propose a living review that continuously tracks public datasets and their associated research artifacts across multiple medical imaging applications. Our approach includes a framework for the living review to monitor data documentation artifacts, and an SQL database to visualize the citation relationships between research artifact and dataset. Lastly, we discuss key considerations for creating medical imaging datasets, review best practices for data annotation, discuss the significance of shortcuts and demographic diversity, and emphasize the importance of managing datasets throughout their entire lifecycle. Our demo is publicly available at this http URL.

02 Oct 2024

The various limitations of Generative AI, such as hallucinations and model failures, have made it crucial to understand the role of different modalities in Visual Language Model (VLM) predictions. Our work investigates how the integration of information from image and text modalities influences the performance and behavior of VLMs in visual question answering (VQA) and reasoning tasks. We measure this effect through answer accuracy, reasoning quality, model uncertainty, and modality relevance. We study the interplay between text and image modalities in different configurations where visual content is essential for solving the VQA task. Our contributions include (1) the Semantic Interventions (SI)-VQA dataset, (2) a benchmark study of various VLM architectures under different modality configurations, and (3) the Interactive Semantic Interventions (ISI) tool. The SI-VQA dataset serves as the foundation for the benchmark, while the ISI tool provides an interface to test and apply semantic interventions in image and text inputs, enabling more fine-grained analysis. Our results show that complementary information between modalities improves answer and reasoning quality, while contradictory information harms model performance and confidence. Image text annotations have minimal impact on accuracy and uncertainty, slightly increasing image relevance. Attention analysis confirms the dominant role of image inputs over text in VQA tasks. In this study, we evaluate state-of-the-art VLMs that allow us to extract attention coefficients for each modality. A key finding is PaliGemma's harmful overconfidence, which poses a higher risk of silent failures compared to the LLaVA models. This work sets the foundation for rigorous analysis of modality integration, supported by datasets specifically designed for this purpose.
13 Aug 2025
X-ray computed tomography (CT) is the main 3D technique for imaging the internal microstructures of materials. Quantitative analysis of the microstructures is usually achieved by applying a sequence of steps that are implemented to the entire 3D image. This is challenged by various imaging artifacts inherent from the technique, e.g., beam hardening and partial volume. Consequently, the analysis requires users to make a number of decisions to segment and classify the microstructures based on the voxel gray-values. In this context, a software tool, here called ARI3D, is proposed to interactively analyze regions in three-dimensional X-ray CT images, assisting users through the various steps of a protocol designed to classify and quantify objects within regions of a three-dimensional image. ARI3D aims to 1) Improve phase identification; 2) Account for partial volume effect; 3) Increase the detection limit and accuracy of object quantification; and 4) Harmonize quantitative 3D analysis that can be implemented in different fields of science.

23 Aug 2022
Semantic segmentation is one of the most popular research areas in medical image computing. Perhaps surprisingly, despite its conceptualization dating back to 2018, nnU-Net continues to provide competitive out-of-the-box solutions for a broad variety of segmentation problems and is regularly used as a development framework for challenge-winning algorithms. Here we use nnU-Net to participate in the AMOS2022 challenge, which comes with a unique set of tasks: not only is the dataset one of the largest ever created and boasts 15 target structures, but the competition also requires submitted solutions to handle both MRI and CT scans. Through careful modification of nnU-net's hyperparameters, the addition of residual connections in the encoder and the design of a custom postprocessing strategy, we were able to substantially improve upon the nnU-Net baseline. Our final ensemble achieves Dice scores of 90.13 for Task 1 (CT) and 89.06 for Task 2 (CT+MRI) in a 5-fold cross-validation on the provided training cases.

10 Apr 2023

Foundation models have taken over natural language processing and image generation domains due to the flexibility of prompting. With the recent introduction of the Segment Anything Model (SAM), this prompt-driven paradigm has entered image segmentation with a hitherto unexplored abundance of capabilities. The purpose of this paper is to conduct an initial evaluation of the out-of-the-box zero-shot capabilities of SAM for medical image segmentation, by evaluating its performance on an abdominal CT organ segmentation task, via point or bounding box based prompting. We show that SAM generalizes well to CT data, making it a potential catalyst for the advancement of semi-automatic segmentation tools for clinicians. We believe that this foundation model, while not reaching state-of-the-art segmentation performance in our investigations, can serve as a highly potent starting point for further adaptations of such models to the intricacies of the medical domain. Keywords: medical image segmentation, SAM, foundation models, zero-shot learning
09 Jan 2024

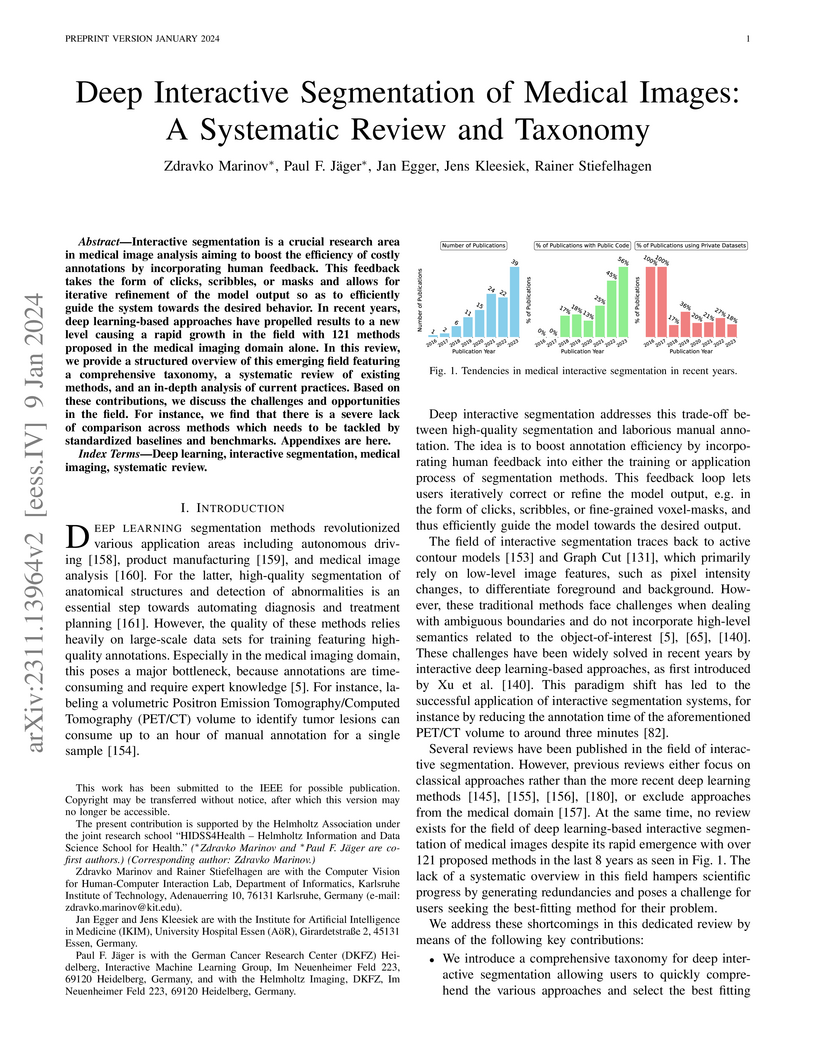
Interactive segmentation is a crucial research area in medical image analysis aiming to boost the efficiency of costly annotations by incorporating human feedback. This feedback takes the form of clicks, scribbles, or masks and allows for iterative refinement of the model output so as to efficiently guide the system towards the desired behavior. In recent years, deep learning-based approaches have propelled results to a new level causing a rapid growth in the field with 121 methods proposed in the medical imaging domain alone. In this review, we provide a structured overview of this emerging field featuring a comprehensive taxonomy, a systematic review of existing methods, and an in-depth analysis of current practices. Based on these contributions, we discuss the challenges and opportunities in the field. For instance, we find that there is a severe lack of comparison across methods which needs to be tackled by standardized baselines and benchmarks.
02 Jan 2025

Explainable AI (XAI) is a rapidly growing domain with a myriad of proposed
methods as well as metrics aiming to evaluate their efficacy. However, current
studies are often of limited scope, examining only a handful of XAI methods and
ignoring underlying design parameters for performance, such as the model
architecture or the nature of input data. Moreover, they often rely on one or a
few metrics and neglect thorough validation, increasing the risk of selection
bias and ignoring discrepancies among metrics. These shortcomings leave
practitioners confused about which method to choose for their problem. In
response, we introduce LATEC, a large-scale benchmark that critically evaluates
17 prominent XAI methods using 20 distinct metrics. We systematically
incorporate vital design parameters like varied architectures and diverse input
modalities, resulting in 7,560 examined combinations. Through LATEC, we
showcase the high risk of conflicting metrics leading to unreliable rankings
and consequently propose a more robust evaluation scheme. Further, we
comprehensively evaluate various XAI methods to assist practitioners in
selecting appropriate methods aligning with their needs. Curiously, the
emerging top-performing method, Expected Gradients, is not examined in any
relevant related study. LATEC reinforces its role in future XAI research by
publicly releasing all 326k saliency maps and 378k metric scores as a
(meta-)evaluation dataset. The benchmark is hosted at:
this https URL
There are no more papers matching your filters at the moment.
